Have you ever felt like you sweat more than those around you? Maybe you noticed that your shirt gets soaked in the gym while others tend to stay the same color. Perhaps you get a wave of embarrassment during times that require you to shake someone’s hand or raise your arms. If this sounds familiar, don’t be ashamed! You may suffer from hyperhidrosis, a relatively common condition affecting approximately 15.3 million people in the US alone! This condition can cause a lot of anxiety for patients. The good news is that it is not medically serious (yet underlying causes of increased sweating that may be harmful should be ruled out first) and there is a large variety of treatments available to help you get back to feeling comfortable and stress-free!
Understanding Hyperhidrosis
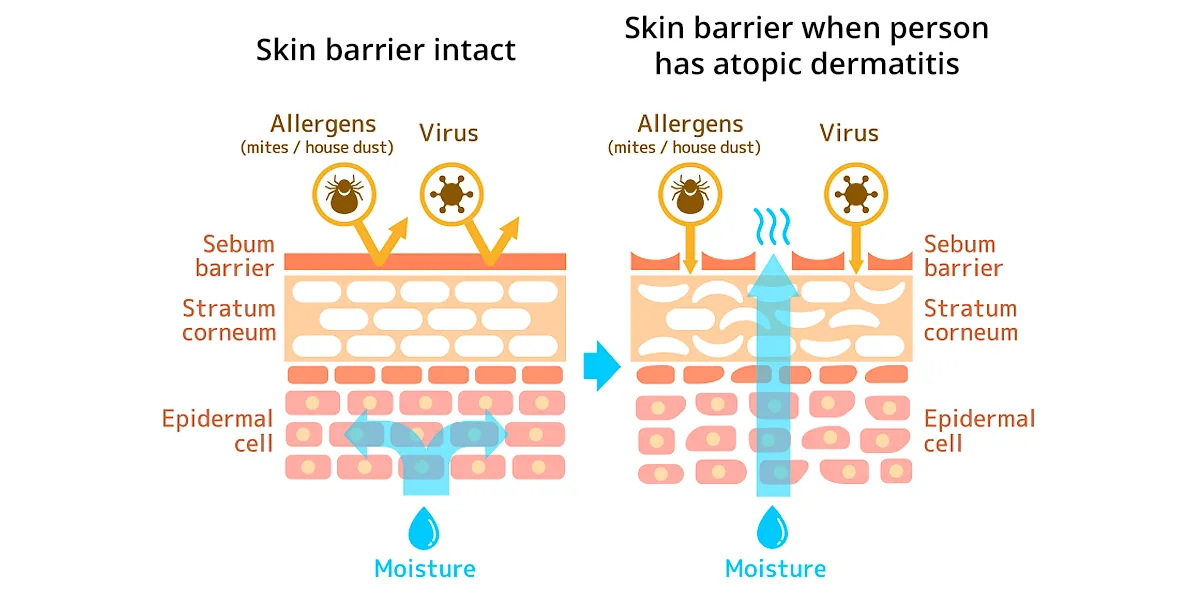
Patients suffering from hyperhidrosis may look at the process of sweating as awful, but it is actually a natural and necessary bodily function. Sweating is part of our body’s repertoire for regulating our temperature. Sweating is our most powerful autonomic thermoeffector! When we start to “overheat,” our bodies respond by covering the skin in sweat. The evaporation of this sweat provides the greatest potential for heat loss, and is the only mechanism by which we can lose heat when air temperature is greater than that of the skin. Unfortunately, in the case of those with hyperhidrosis, it can become a daily struggle that affects their mental health and well-being.
Hyperhidrosis is caused by an overstimulation of cholinergic receptors on eccrine glands. These eccrine glands are concentrated in areas like the armpits, palms, soles, and face, hence why these areas are key places to see hyperhidrosis. Although the process of sweating is physiologic, it becomes pathologic in these individuals due to an impaired acetylcholine negative feedback loop. This excess sweating can be triggered by stress, anxiety, fear, nervousness, and even from no cause at all. It affects both men and women equally. The condition is usually diagnosed within the first three decades of life, but palmar and axillary hyperhidrosis tend to be diagnosed earlier in childhood and adolescence.
Types of Hyperhidrosis
There are two types of hyperhidrosis, primary and secondary. Each is managed quite differently, making it important for your provider to diagnose you correctly. The etiology of primary hyperhidrosis is still unknown. Genetic factors are thought to play a role in the increased neural stimulation that occurs involving the eccrine glands, but this is not fully understood. Secondary causes of hyperhidrosis, hence why we call it secondary hyperhidrosis, are easier to identify since we know about the association between the cause and increased sweating. Some of these causes are medications, systemic diseases, and various tumors. Illnesses that cause a fever can also lead to hyperhidrosis as a means to cool off the increased body temperature. However, the rest of this article will primarily focus on primary hyperhidrosis, as this is what we classically think of when we see a patient presenting to the dermatologist’s office for treatment.
Primary hyperhidrosis is a benign condition, but underlying causes of the condition must always be ruled out due to the multitude of serious medical problems that can cause an increase in sweating. For example, a patient coming in with hyperhidrosis late in life would be more likely to be suffering from a more serious condition than a younger patient complaining of the same issue. The medical workup involves a more focused history and physical pertaining to the sweating. Patients may have blood work ordered depending on their examination. For instance, a patient with symptoms of withdrawal and a history of opioid use would lead us towards suspicion that this is a secondary hyperhidrosis. As you can see, the causes of secondary hyperhidrosis can seem endless! Luckily, for primary hyperhidrosis, the International Hyperhidrosis Society created an ABC’s of the condition to help identify factors that strongly suggest primary hyperhidrosis.
Treatment Options
With so many treatments for hyperhidrosis, it may seem confusing on where exactly to begin. The best approach is a stepwise one, starting with over-the-counter options when applicable, and trying more invasive options if the initial choices fail.
Over-the-Counter Solutions: The first-line treatment for hyperhidrosis is over-the-counter aluminum chloride hexahydrate 20%. It is usually used for 3 to 4 nights in a row and then nightly as needed. The aluminum chloride works by obstructing the distal sweat gland ducts. Ideally, patients use a higher concentrated product than the standard percentage found in regular antiperspirants; 15% aluminum chloride solution is the minimum recommended. Another newer topical option is glycopyrronium tosylate, which is a cloth “wipey” product premoistened with a 2.4% glycopyrronium solution.
Oral Medications: After failing topical treatments or for when there is more widespread sweating, your provider will likely give oral anticholinergic medications a shot. This includes oxybutynin or glycopyrrolate. The biggest downside to these anti-cholinergic agents is that the cholinergic receptors they block do more than just cause sweating! Stimulation of these receptors allows us to keep our eyes and mouth moist, use the bathroom without issue, and much more! It makes sense then that by blocking these pathways, we see side effects like dry mouth and eyes, urinary retention, constipation, and a number of other issues. All patients are unique and respond differently to medications, so do not let these side effects sway you from ever giving these medications a chance!
Iontophoresis: A well-researched, but less commonly used method due to inconvenience is iontophoresis. Two to three sessions are done per week. This method is best used for palmar and plantar hyperhidrosis since it is difficult to target the armpit. It is not fully understood how iontophoresis works at reducing sweating, but a number of theories exist.
Botulinum Toxin: Botulinum toxin is another option that involves expensive, repeated injections of the toxin into the area suffering from hyperhidrosis. The toxin’s known effect of cleaving SNAP-25 protein and stopping the binding and presynaptic vesicle fusion of acetylcholine with the nerve terminal leads to a decrease in acetylcholine release. The mechanism’s end effect is essentially the same as anti-cholinergic drugs: the signal to cause sweating in our bodies is being cut off.
Surgical Procedures: There are several surgical procedures for hyperhidrosis, with a few that have been developed more recently. Affected areas can undergo radiofrequency ablation, long pulse lasers, thermal energy, subcutaneous liposuction, and even surgical excision. The exact treatment depends on the area, as options like radiofrequency ablation and thermal energy are not approved for areas besides the armpits. When all else fails, patients can elect to undergo sympathectomy. This involves excising the sympathetic ganglia responsible for sweating.
As you can see, while primary hyperhidrosis is not a life-threatening condition, it can be mentally debilitating. The impact it has on everyday activities can put a hamper on one’s social life and cause great amounts of stress. Fortunately, there are a number of treatments available, with the majority being non-invasive. The success of these treatments varies quite a bit from person to person, but the good news is that there is plenty treatment options for this condition.